Health Drivers Research
Increasing Health Drivers Cancer Control Research to Achieve Health Equity
The elimination of cancer-related disparities is an important goal for DCCPS. Health drivers (HD) are the adverse effects on populations who have systematically experienced greater obstacles to health based on factors such as race and ethnicity, gender, age, religion, socioeconomic status, education, disability, geographic location, sexual identity, gender identity, or other characteristics historically linked to discrimination or exclusion. While health disparity research focuses on the challenges different groups face in achieving the highest level of health possible, health equity (HE) is the attainment of the highest level of health for all people. Achieving health equity requires valuing everyone equally, with focused and ongoing societal efforts to address avoidable inequalities, historical and contemporary injustices, and the elimination of health and healthcare disparities.
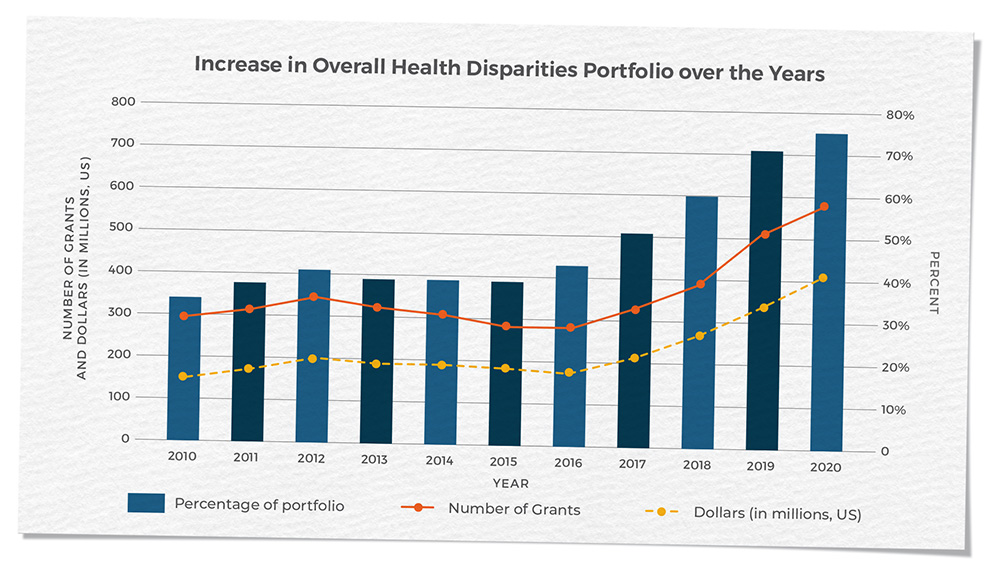
DCCPS’s commitment to addressing health drivers in cancer control has resulted in an extensive portfolio of grants spanning from longitudinal cohort studies to epidemiological studies, healthcare delivery research, social and behavioral intervention research, omics research, and surveillance studies. The division has dedicated efforts to increasing the cancer control health drivers and health equities funded research portfolio and, in recent years, has seen a tremendous increase in the number of health drivers and health equity grants within the total division grant portfolio. In FY 2020, approximately 76% of the division’s funded awards included a health drivers component.
Source: National Cancer Institute. Health Drivers Research Grants Funded in the US
Available at: https://maps.cancer.gov/overview/map/index.jsp?grantType=5&raId=2&fy=1998&programId=undefined
Expanding the Portfolio
The growth in the number of HD/HE grants is primarily due to the expansion of programs focusing on various medically underserved populations. The RESPOND Study, Research on Prostate Cancer in African American Men: Defining the Roles of Genetics, Tumor Markers, and Social Stress, is the largest coordinated research effort to study biological and non-biological factors associated with aggressive prostate cancer in African American men. This research is vital to address the prostate cancer disparities that currently exist: African American men are over 75% more likely to be diagnosed with prostate cancer and more than twice as likely to die of prostate cancer compared to other racial/ethnic groups. Similar disparities are shown with cancer incidence and mortality rates for other cancers such as breast, colorectal, and lung cancers, with African Americans more likely to be diagnosed with more-advanced-stage disease and experience higher cancer mortality rates than other groups. The Detroit Research on Cancer Survivors study focuses on the major factors affecting cancer progression, recurrence, mortality, and quality of life among African American cancer survivors in the largest study to date of African American cancer survivors in the United States.
Concerted efforts to enhance research capacity in rural and remote areas through multiple funding opportunities and networks have led to the creation of many new partnerships between researchers and NCI-Designated Cancer Centers, with community stakeholders, and with rural healthcare delivery partners. Populations living in rural areas have higher average death rates for all cancer sites combined, compared to populations in urban counties, and have higher incidence and death rates for cancers caused by smoking (e.g., lung and laryngeal cancers) and higher rates of incidence of cancers that can be prevented by screening (i.e., colorectal and cervical cancers). To reduce and ultimately eliminate rural cancer-related health drivers, DCCPS has collaborated with HRSA, USDA, the National Center for Health Statistics, CDC, and the US Census Bureau — agencies who have spent many years working with rural communities — and who have provided the division with valuable information and insights on how to address rural health drivers.
Funding opportunities have invited investigators to conduct research in these rural communities of greatest need. The Rural Supplements to NCI-Designated Cancer Centers were funded in FYs 2018 and 2019, with the goal of developing research capacity and feasibility on rural cancer control through collaboration with rural clinics, data collection and integration, and studying the implementation of research programs. Many awardees of this supplement went on to receive funding for more extensive work in rural communities, including those awarded grants from the “Improving the Reach and Quality of Cancer Care in Rural Populations” RFA, and the recent NOSI for administrative supplements focused on Research in Geographically Underserved Areas. In addition, the current “Social and Behavioral Intervention Research to Address Modifiable Risk Factors for Cancer in Rural Populations” RFA seeks research applications that develop, adapt, and test interventions to address social and behavioral modifiable risk factors for cancer in rural populations. The recent release of the Rural-Urban Disparities in Cancer map story provides a geographic portrayal of cancer burden among populations that reside in rural versus urban areas, drawing upon the recent research findings related to rural disadvantage and summarizing the division’s efforts to improve the outcomes of cancer in rural areas.
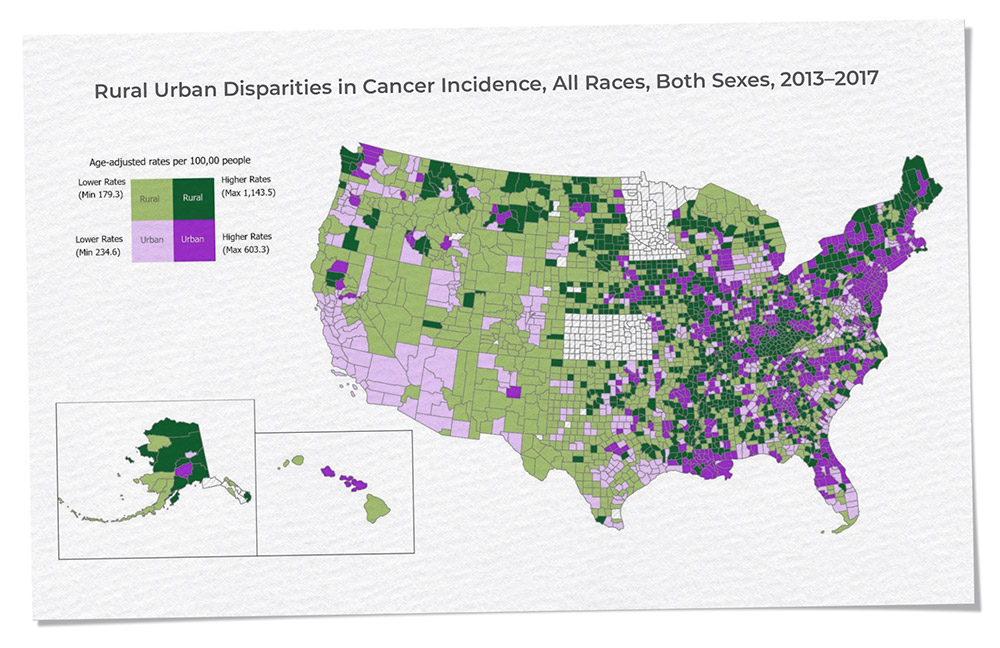
Source: National Vital Statistics System (https://www.cdc.gov/nchs/nvss/index.htm?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fnchs%2Fnvss.htm) at the National Center for Health Statistics, Centers for Disease Control and Prevention.
Rural-urban county classification is based on 2013 USDA Rural-Urban Continuum Codes.
American Indian and Alaska Native (AI/AN) populations are among the underserved minority groups in the US disproportionately affected by certain cancers, with the lowest survival rates for nearly all types of cancer of any subpopulation and cancers often detected at later stages. The Intervention Research to Improve Native American Health (IRINAH) program was created in 2011 to develop, adapt, and test the effectiveness of health-promotion and disease-prevention interventions in Native populations, and over the years has funded 35 projects from across multiple NIH institutes, with four projects focusing on cancer research. A Native American Cancer Control Literature Database was developed in conjunction with the IRINAH program and has now expanded to include over 1,700 scientific publications on cancer-related topics with Native American communities, including AI, AN, Native Hawaiian, and First Nations populations. Another intervention project is the “Dissemination of a Colorectal Cancer Screening Program Across American Indian Communities in the Southern Plains and Southwest United States Consortia,” which consists of three NCI-Designated Cancer Centers that are funded through the Cancer Moonshot. The goal of this research effort is to enhance health equity through the reduction of colorectal cancer disparities in morbidity, mortality, stage at diagnosis, and increased survival among AIs through the implementation of multilevel interventions.
We have made substantial progress in our understanding of cancer disparities and inequity over the past few decades. Future advances require expansion into more tailored research focused on medically underserved populations. DCCPS will continue to support HD/HE research to address barriers faced by medically underserved populations and to improve cancer care prevention and delivery conditions research, ultimately working toward eliminating all cancer-related disparities.
Continue To